Sprained Ankle – How to Recover
Have you ever experienced the immediate searing pain from a rolled or sprained ankle? How about repeated experiences of this? Or are you the person who has rolled their ankle/s so many times now that it happens daily, with no obvious challenge? Chances are most of you have had the first of second experience but unfortunately for many people the third is their reality. Ankle sprains or rolling your ankle is one of the most common sporting related injuries. A sudden wrong step can lengthen or worse tear the ligaments that support the ankle. To give yourself the best chance of avoiding progression to chronic instability, early intervention and progression of demands for a sprained ankle is the key.

What happens when you sprain or roll your ankle?
By spraining or rolling your ankle, the soft tissue that supports the ankle, known as ligaments which are attached on 2 separate bones, can be stretched due to an external force applying excessive force and elongating the ligament. A ligament’s role is to provide stability between 2 bones reducing the ability of the joint to lose position. Unfortunately the ligaments have quite poor elastic properties so once a ligament has been stretched, it doesn’t return back to its original length easily, which subsequently compromises the stability of the joints they hold together.
Not all sprains are the same. So which type of sprain do you have?
How you manage and recover from a sprain will vary depending on the type of sprain. The majority of sprains can be classified into one of two categories:
Inversion Sprain
This is the most common ankle sprain where your ankle rolls out, turning the underside of foot inwards, placing all the weight on the outside of the foot/ankle stretching the ligaments on the lateral (outside) side of the ankle and foot. This is common with change of direction or side to side movements or in court sports where you need to abruptly stop sideways movement eg. tennis, squash, netball, basketball. This generally results in swelling around the outside and top of the ankle. Depending on the severity of the sprain can range for general tenderness difficulty weight bearing right through to complete lack of ability to tolerate any load/weight on the foot and ankle.
Eversion Sprain
This ankle sprain does not occur as often as the inversion sprain however can often be more severe when it does occur. This ankle sprain is where the ankle is rolled inward toward the instep causing the sole of the foot to turn outwards. As a result all the weight is forced to the inside of the ankle stretching the medial (inside) ligaments of the ankle. This type of sprain is more common in contact sports, snow sports and activities such as skateboarding. Because of the mechanics of an eversion sprain there is often risk of concurrent injuries at the knee when sustaining an eversion sprain.
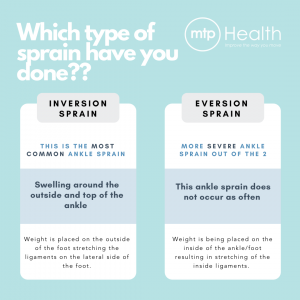

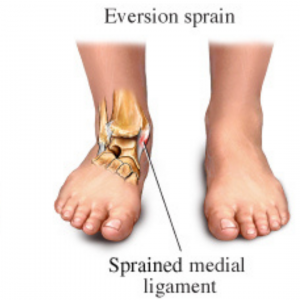
Image credit: https://www.physio-pedia.com
What to do once you have sprained your ankle?
We have often referred to the first aid acronym RICE (Rest, Ice, Compress and Elevation) in the effort to try and slow the immediate levels of swelling and inflammation that occurs around the ankle. However, this model has drawn criticism in recent years due to the implications of cold and elevation reducing the blood flow and therefore slowing the healing process that the body will naturally go through, possibly resulting in longer time to full recovery and return to pre-injury state.
At MTP Health we apply both philosophies depending on the presentation. Often when there is a traumatic sprain (for example on resulting in tearing of the ligaments rather than simply stretching them) the body will over-react in its inflammatory response. So the applying the RICE method immediately to regulate this over-reaction can expedite their ability to progress back to movement based rehabilitation. However we would cease applying ice/anti-inflammatory after the emergency application in preference of the “P.E.A.C.E and L.O.V.E” approach.
Like everything we do at MTP Health our approach is about long term outcomes. So how does this impact the long term results. Well, if we focus too much on the acute management and avoid loading or movement then we run the risk of weakening or atrophy of the muscles around the ankle. The weaker we get the more unstable our ankle will become and the more likely we are to sustain another ankle sprain! This can also lead to other compensatory injury up the kinetic chain (eg. knees, hips or backs) where these joints are required to compensate for the weakness of the ankle.
So rather than RICE method MTP Health Exercise Physiologists help our clients to manage their sprained ankles is with “PEACE and LOVE”. These 2 acronyms explain both the acute management phase and long-term management phase to reduce the risk of re-injury and return to pre-injury state.
PEACE
P = Protect
Protecting the ankle from further damage is the number one priority when beginning the acute phase of rehabilitation. This involves restricting the movement for 1-3 days to minimise bleeding and reduce the risk of aggravating the injury. Rest however should be minimised as this can compromise tissue strength and quality.
E = Elevate
Elevating the ankle so that it is above the heart will promote interstitial blood flow from the ankle thus possibly reducing the amount of swelling that will occur around the ankle.
A = Avoid Anti-Inflammatory Modalities
Inflammation is the bodies way of repairing damaged tissues. So, when we use anti-inflammatories, we are restricting the bodies main mechanism to heal the tissues that have been damaged because of the sprain which then can have long term affects.
C = Compress
By providing an external mechanical structure over the first 1-3 days such as taping or splinting, this can reduce the ability of the injured soft tissue to haemorrhaging.
E = Educate
Education about the mechanism of the injury and how to rehabilitate is vital in the rehabilitation of an ankle. Letting our clients know of what to do and what not to do time it takes to completely recover and the possible solutions there are, will give the client a better understanding of expectations and what needs to be done to have a successful rehabilitation.
LOVE
L = Load
Optimal loading without exacerbating the pain should be done as soon as possible to promote repair, remodelling tissues and increase in tissue tolerance such as ligaments, muscles and tendons.
O = Optimism
This part is more of a psychological factor where if the patient has a more optimistic approach to recovery, it has been shown to have a more positive result towards the recovery.
V = Vascularisation
Undergoing cardiovascular activity whilst pain free is vital in rehabilitating a sprained ankle. This aerobic type of activity should occur a few days after the sprain has occurred to increase the blood flow around the ankle joint and thus function of the ankle increases.
E = Exercise
Exercise is an important step in restoring mobility, stability, strength, proprioception and most importantly, reducing the risk of re-injury. Pain should be used as a guide on when to progress with the exercises.
What type of Exercises should you be doing?
Like most things this comes with a big asterix*… You should seek professional advice from your Exercise Physiologist, Physio or Doctor. But to give you an idea of a simple starting point for movement once you have managed the very acute phase of your sprain.
1. Active Range of Motion
- Plantarflexion & Dorsiflexion: Simple forward and backward movement trying to point toes then pull toes as far back as possible.
- Inversion & Eversion: Turning your foot in and out, focus on gentle movement without changing your knee and hip position.
- Circumduction: Circular motion incorporating all directions of movement. Demonstrated below as a Controlled Articular Rotation (CAR)
2. Light Resisted Movement
- Theraband Plantar & Dorsi Flexion: Using band resistance to increase the tension/load to ensure the muscles are working nicely at the front and back of ankle without aggravating (shown in 4 way video below)
- Theraband Inversion/Eversion: In and out rotation as demonstrated below.
- Heel Raises: Either seated or standing depending on level of discomfort, press through the toes and forefoot to lift heels off the floor, keeping pressure through base of big toe
- Tibialis Raises: With your back to a wall, pull your toes back toward you and lift your forefoot off the floor. Keeping the heels in contact with the ground and legs straight.
3. Balance and Control
- Pillow or Cushion Balance: Progressions. Note, only complete the level at which you are capable and safe. Aim to be confident in each position for 15-30seconds before progressing to the next movement.
- Single Leg Eyes Open
- Single Leg Eyes Closed
- Single Leg Look Around
- Single Leg Forward Backward Reach
- Single Leg Side to Side Reach
- Single Leg Rotation Balance
Getting the best results
It is most important that the treatment is correctly prescribed to prevent the chance of re-injuring (check out our 2 part blog on preventing re-injury) which could result in a longer-term injury than the original. The safest and most effective way to achieve a positive result is through an individualised exercise program designed by a professional. Our Exercise Physiologists use up to date evidence and undergo a thorough assessment when you arrive to be able to design and deliver the best exercise prescription and advice possible. We strive to achieve not only a positive result, but we want you to be stronger than when you were before to be able to reduce the chance of another ankle sprain from happening again.